
Actually, most patients don’t. A recent study conducted by Catalyst Healthcare Research found that 93% of adults would prefer to go to a doctor that offers email communication, even if there was a $25 fee (Pai, 2014). Encrypted email is incorporated into most, if not all present-day EHRs (Electronic Health Records) that also have patient portals. By being integrated with the entire medical record, it’s relatively easy for doctors to correspond with patients right from their electronic chart. Leaders in prominent health care groups in Houston, encouraged patient enrollment in their EHR system and have found similar results. Dr. Robert Dickinson, Kelsey-Seybold’s medical director for executive health and wellness says, “They think it’s the coolest thing they’ve ever seen. It’s like online banking. People love this kind of access. Before, it was kind of mysterious” (Hines, 2014).
However, when you ask doctors if they like EHRs, you often get an entirely different story. You mostly hear dislike, frustration and irritability. There are actually excellent reasons for this. To begin the discussion, we have to go back to the Meaningful Use days. For those who may not know, the Meaningful Use legislation grew out of the HITECH act of 2009 as a way to promote interoperability among EHRs. The eventual goal was to create a national database that would hold each U.S. resident’s healthcare data. The goal, in my opinion, was not really a bad one. However, the way they went about doing it was only slightly short of disastrous. To encourage nationwide adoption of EHRs, physicians and healthcare systems were offered huge financial incentives. Simultaneously, both Medicare and Medicaid providers were expected to show that they were “meaningfully using” their EHRs to meet certain standards that were presumed to at least measure and hopefully also ensure good treatment outcomes. More importantly, if providers did NOT meet these standards, their reimbursements were dinged. Naturally, there was a huge push by physicians to obtain EHRs and begin recording the measures that were now required to prevent loss of income. At first, the fact that they were being incentivized to purchase EHR systems sweetened the pot substantially.
On the other end of things, software developers saw a huge opportunity: almost the entire U.S. healthcare system suddenly wanted/needed EHRs and had plenty of money to pay for them, thanks to the financial incentives provided by the government. There was a huge race to get products out the door QUICKLY to beat out the competition for a larger share of the healthcare pie. This set several unfortunate processes in motion. First, no one said these products had to be good or easy to use. They just had to meet certain requirements (written by the federal government) which would presumably lead toward national interoperability and also allow providers to meet their Meaningful Use requirements. The race was on: doctors and healthcare systems wanted EHRs; developers wanted to build EHRs as quickly as possible before the incentive well dried up. The second HUGE problem with all of this is that the federal government was telling both physicians and software developers how to do their jobs via the mandates. The real professionals in these fields had their hands tied and felt unable to do the kind of quality work for which they had been trained.
The results were what you would expect. Many of the EHR programs were clunky and difficult to use. Doctors felt the things they were being required to measure and record were, in many cases, meaningless instead of meaningful. Furthermore, they were being required to record this data in programs that were annoying and often wasted more time than they saved. They complained that EHRs caused them to be less engaged with their patients and that, overall, they were a hindrance to actually providing solid patient care. So yes. Doctors grew to hate their EHRs. Some hated them so much that they ditched them, either deciding to no longer be providers for Medicare and/or Medicaid or at least to stop reporting the things they felt were non-helpful timewasters and just accept the financial penalties.
Enter behavioral health. And this is where it gets interesting. There were huge debates over whether those of us in the behavioral health fields should or should not be mandated into Meaningful Use. Even among behavioral health providers and their professional agencies, there was disagreement, with some strongly advocating for us TO be included, and others advocating equally as strongly for us NOT to be included. The eventual outcome was that those of us in behavioral health professions were NOT included in the Meaningful Use legislation. We were not required to start using EHRs. We could continue to use our paper-pencil methods or whatever else we chose. What this allowed was an opening for another whole breed of software developer, often behavioral health providers themselves, who had an interest in ONLY developing products for the mental health field. Since there were no mandates, developers of these products – PSYBooks being one example – were free to concentrate on building EHRs according to the best standards of their profession, as they had been trained. The federal government was not telling them how to do their job. However, the downside was that the federal government was ALSO not incentivizing behavioral health practitioners to buy these products. Subscribers had to pay the fees for these EHRs out of their pockets. The end result was that developers of these types of EHRs – the “non-certified” EHRs built primarily for behavioral health – HAD to build products their users liked if they wanted to stay in business. The race was not to build a product that adhered to standards written by policymakers who knew little about either healthcare or software development, but rather, to build products therapists really enjoyed using. Products that really DID save people time and make their jobs easier.
These non-certified EHRs also have to adhere to all HIPAA standards. They are as fully compliant as certified EHRs. However, when your focus is on building a product people like, you begin by looking at what they DON’T like in the other products and then find different ways to solve the same problem. A good example of this is what’s been called the “walled garden” approach taken by certified EHRs. This approach categorizes each user of the system according to their role in the company. In other words, schedulers can schedule, billers can bill, doctors can write orders and so on. One of the frustrations doctors often express is, for example, if the patient is sitting right there and they want to schedule a follow-up session, they’re not permitted by the system to do it. They’re not a scheduler. So they have to send the patient to the scheduler or give the patient a number to call to get themselves scheduled, which may or may not be a time the doctor wanted. If, for example, the doctor intended to fit the person in the next day for a quick follow-up, the scheduler would not know that. They might look at the doctor’s calendar and see that it was full. This means that the doctor now has to take more time out of their schedule to contact the scheduler to tell them what they want done. In PSYBooks and other similar kinds of products, this problem is dealt with differently. HIPAA mandates that each person in the company should only be allowed to view the portion of the patient’s chart they actually need to carry out their duties. But, instead of the program making these kinds of determinations for your practice, in programs like PSYBooks, each provider makes those decisions for themselves. You set the permissions for each employee, contract worker or supervisee in your practice. By default, providers have access to everything. It is their practice so they get to decide how they want to set up their EHR.
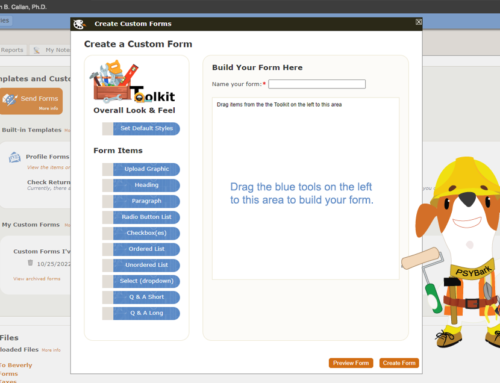
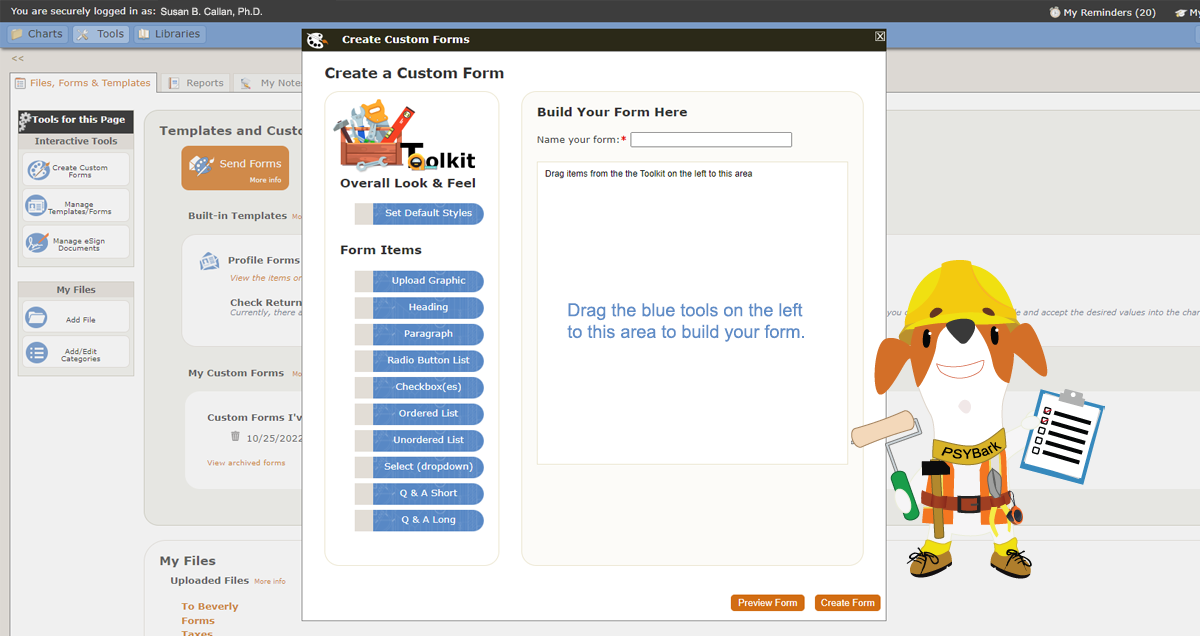
The above is only one example but it’s meant to illustrate the process of us listening to what YOU want and need, then taking our knowledge of both software development and healthcare rules and mandates such as HIPAA to build a product that you can enjoy using. If you’re not happy with your current EHR, or if you’re considering making the switch from paper to electronic recordkeeping, please check us out. We’d love to show you around.
Girgis, L. (2017, July 19.) Why Doctors Hate Their EHRs. Physicians Practice. https://www.physicianspractice.com/view/why-doctors-hate-their-ehrs
Pai, A. (2014, June 03.) Survey: Patients prefer doctors who offer email communication. https://www.mobihealthnews.com/33265/survey-patients-prefer-doctors-who-offer-email-communication


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}